Surgical Lip Repositioning Procedure for the
Reconstruction of Pink Esthetics in a Periodontal
Way: A Case Report
Dr. Bushra K Quazi*1, M.D.S., Dr. Manohar Laxmanrao Bhongade1, Dr. Bhumika Sehdev2
1Department of Periodontics and Implantology, Sharad Pawar Dental College, Wardha, Maharashtra
2Department of Periodontics, R R Dental College and Hospital, Umarda District, Udaipur, Rajasthan, India)
Abstract:
Cosmetic procedures involving reconstruction of gingivae have become an integral part of current periodontal practice. The
ability to cover unsightly exposed teeth and recontour soft tissue by reducing the excessive gingival display have added an esthetic
angle to the traditional concept of biological and functional periodontal health. Excessive gingival display can be managed by a
variety of treatment modalities, depending on the specific diagnosis. Lip repositioning surgery is a largely unknown and
underutilized treatment modality for excessive gingival display. Lip repositioning is a simple non-invasive surgical procedure to
treat ‘gummy smile’. It restricts the muscle pull of the elevator lip muscles thereby reducing the gingival display while smiling.
This procedure is safe and predictable with minimal risk or side effects. The aim of the present case report was to minimize
excessive gingival display with a lip repositiong procedure; thereby reconstructing the pink esthetics in a periodontal way. The lip
repositioning technique to decrease the amount of gingival display proved to be more conservative and provided good esthetic
outcome.
Excessive gingival display, gummy smile, lip repositioning.
Introduction
The harmony of the smile is determined not only by the shape, the position, and the colour of teeth but also by the gingival tissues. Excessive gingival display (EGD), which is
commonly described as „gummy smile‟ adversely affectssmile aesthetics and therefore undesirable. It is one of the several developmental or acquired deformities and
conditions that manifest in the periodontium.[1] It is an aesthetic concern that can affect a large portion of thepopulation, with a reported prevalence between 10.5% and29%.[2,3] In the recent years, EGD has received an increased emphasis in dental literature and various treatment optionsare now available for correction of gummy smile.
Excessive gingival display has four possible etiologies. First, it may be a result of delayed eruption in which the gingivae fail to complete the apical migration over the maxillary teeth to a position that is 1 mm coronal to the cement-enamel junctions.[4,5] In these patients, restoring the normal dentogingival relationships can be achieved with an esthetic crown lengthening, which is a well-documented treatment modality that is highly effective in treating patients with delayed eruption.[6,7] The second possible cause is compensatory eruption of the maxillary teeth with
concomitant coronal migration of the attachment apparatus, which includes the gingival margins. Orthodontic leveling of the gingival margins of the maxillary teeth may beconsidered in this situation.[8] Resective surgery is also possible but may expose the narrow root surface and necessitate a restoration. The third possibility is vertical maxillary excess in which there is an enlarged vertical dimension of the midface and incompetent lips. Treatment involves orthognathic surgery to restore normal inter- jaw relationships and to reduce the gingival display;[9] this
involves hospitalization and significant side effects for patients.
Finally, when the patient smiles, if the upper lip moves in an apical direction and exposes the dentition and excessive gingivae, then surgical lip repositioning may be utilized to reduce the labial retraction of the elevator smile muscle and minimize the gingival display. This procedure was first described in the plastic surgery literature in 1973[10] and was recently published in the dental literature.[11] During patient examination, it is important to establish the etiology responsible for the excessive gingival display.
Corresponding Author –
Dr. Bushra.K Quazi
P.G. Department of Periodontics, Sharad Pawar Dental
College, Sawangi (M), Wardha – 442005
Email id – bushrakq27@gmail.com
International Journal of Innovative Research in Medical Science (IJIRMS)
The objective of lip repositioning is to limit the retraction of elevator smile muscles. Lip repositioning results in shallow vestibule restricting the muscle pull thereby limiting thegingival display during smiling. The objectives of this article are to present a case in which the surgical techniqueof “lip repositioning” was used to reduce gingival display, to suggest the technique‟s use as an alternative treatmentmodality; thereby reconstructing the pink esthetics in aperiodontal way.
weeks post operatively. Patient reported mild pain and tension while smiling during the first week after surgery. Loose sutures were removed over a period of four weeks and the remaining sutures are left to be resorbed on their own. Follow-up examinations revealed reduced gingival display. Suture line healed in the form of a scar which was covered by labial mucosa and therefore not visible on smiling.
Case Report
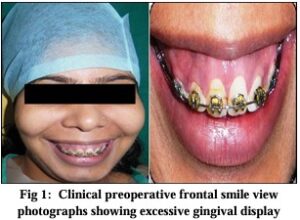
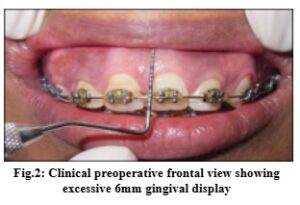
A 19‑year‑old female patient undergoing orthodontic treatment, presented with the complaint of gummy smile following retraction of maxillary anterior teeth (Figure 1) The patient‟s medical history was noncontributory with no contraindication for surgery. Clinical examination revealed moderate amount of maxillary gingival display. With full smile, patient‟s teeth were visible from maxillary right first premolar to maxillary left first premolar with 5-6 mm of gingival display. (Figure 2)Maxillary anterior teeth had normal crown height and width/length ratio. A diagnosis of
moderate vertical maxillary excess was made. Orthognathic surgery as a treatment option was discussed with the patient. However, patient preferred less invasive lip repositioningprocedure over orthognathic surgery. Informed consent was obtained prior to the procedure.
Surgical Procedure
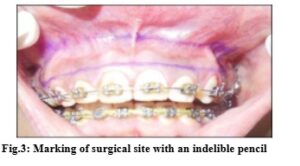
Adequate local anesthetic (lignocaine 2% with epinephrine 1:100,000) was administered in vestibular mucosa and lip from maxillary right first premolar to maxillary left first
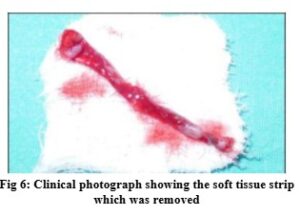
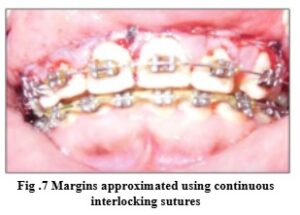
premolar. The surgical site was marked with an indelible pencil (Figure 3). A partial thickness flap was raised frommesial line angle of left maxillary first premolar to the mesial line angle of right maxillary first pre molar at the mucogingival junction (Figure 4). A second incision 10–12mm above the first incision was made in the labial mucosa. The two incisions were joined on either side and a strip of partial thickness flap was removed, exposing the underlyingconnective tissue (Figure 5). The two incisions were then approximated using continuous interlocking sutures (Figure7). Care was taken regarding proper alignment of the midline of the first and second incision lines (lip midline and teeth midline) and avoid any damage to the minor salivary glands in the submucosa. Once the flaps are stabilized, an additional continuing interlocking suture was used to secure complete closure. Pressure was applied until hemostasis was achieved Patient was prescribed nonsteroidal anti‑inflammatory drugs (diclofenac sodium 50mg three times daily for 3 days) and oral antibiotics (amoxicillin 500 mg three times daily for 5 days). Patient
was instructed to apply ice pack post operatively and minimize lip movement for 1 week. Sutures were removed 2

Result
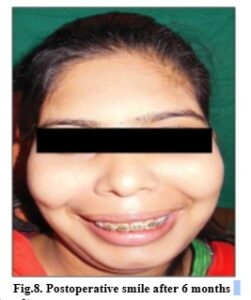
Gingival display at baseline was 5-6 mm which changed drastically at 3 and 6 months postoperatively (Figure 8) At 3 month and at 6 months gingival display was 2 mm. There
was no difference in gingival display between 3 and 6 months.
Discussion
The increase in demand for an attractive smile in the last 40 years resulted in the development of many surgical techniques for correction of the gummy smile. For many people, excessive gingival display is considered undesir¬able. Many factors may play a role in the development of gummy smile including problems related to the gum, the maxilla or the upper lip. A true gummy smile should be differentiated from gingival display related to short clini¬cal crowns or excessive gingival coverage due to delayed teeth eruption. Many procedures were reported in
the literature Fig 6: Clinical photograph showing the soft tissue strip which was removed Fig .7 Margins approximated using continuous interlocking sutures Fig.8. Postoperative smile after 6 months 1246 DOI: 10.23958/ijirms/vol02-i09/01 for managing gummy smile.[12] Such procedures include non-surgical as well as surgical methods such as botulinum toxin injections, crown lengthening, maxillary jaw impaction or orthodontic teeth manipulation. It has been shown that in 20% of patients there is a muscular capacity to raise the upper lip causing gummy smile. In such cases, the myotomy of levator labii superioris can reduce the function of the muscle and decrease the effect of gummy smile.[13,14]
This clinical report describes the use of lip repositioning for the reduction of excessive gingival display. The procedure originated as a plastic surgical treatment but has rarely been described in the dental literature. Variations in lip repositioning have been reported.[15-18] The original technique, did not include severing of the muscle attachment after flap reflection. Other authors advocated performing myectomies to detach the smile muscle attachment.[15-17] The rationale for using myectomies was to allow for tension-free
suturing and to prevent relapse. Contraindications for lip repositioning surgery include inadequate width of attached gingiva in maxillary anterior sextent. Insufficient amount of tissue poses difficulty in flap reflection, stabilization and suturing. Patients with severe vertical maxillary excess cases are also not the ideal candidates for lip repositioning and should be treated with orthognathic surgery.[19]
Silva et al. in 2012 reported successful management of excessive gingival display in a study wherein thirteen patients with excessive gingival display were treated with amodified lip repositioning technique. Treatment consisted of the removal of two strips of mucosa, bilaterally to the maxillary labial frenum and coronal repositioning of the new mucosal margin.The baseline gingival display of 5.8 ±2.1 mm significantly decreased to 1.4 ± 1.0 mm at 3 months and was maintained until 6 months (1.3 ± 1.6 mm). Subjects

were satisfied with their smile after surgery and would likely choose to undergo the procedure again (92%).[20] Similar results were obtained in other case reports by Rosenbaltt,[21]
Simon,[22] and Humayun et al.[23] who achieved approximately 4 mm of reduction in gummy smile.
Jacobs et al. in 2013 reported a case series where seven patients were successfully managed with trial, and then definitive, lip repositioning wherein a mean reduction in gingival display of 6.4 ± 1.5 mm was achieved.[24] Vital et al. in 2013 presented case report of two patientstreated with modified lip repositioning technique and obtained significant improvement in the amount of gingival exposure and esthetic satisfaction after a 6 month follow up.[25] The literature shows only clinical case reports for gummy smile treatment.[25] Several authors have presented case reports of single patients successfully treated with lip repositioning surgery with a follow up period of 6 months.[24]
This case report shows that although the results of lip repositioning surgery appear stable for up to 6 months postoperatively, its utility as a long term treatment option remains questionable. More studies with larger sample size and long term follow‑up are necessary to establish the level of scientific evidence of this procedure.
Conclusion
The positive psychologic effects of improving a patient’s smile often contribute to an improved self-image and enhanced self-esteem. Oral esthetic and functional rehabilitation can be achieved by recontruction of soft tissue in a less invasive periodontal way to an ideal natural form. Surgical lip repositioning is an effective procedure to reduce gingival display by positioning the upper lip in a more coronal location. The long-term stability of the resultsremains to be seen, but it holds promise as an alternative treatment modality in esthetic rehabilitation. Managing gummy smiles with less invasive procedures under local anesthesia can be of a great help to patients. The proposed lip repositioning technique in the current study can be used to correct gummy smiles in patients with gingival display between 4 and 6 mm.